Blog

Author: Mr Chad Chang FRCS(Plast), Consultant Plastic Surgeon
Review Status: Peer-reviewed by Mr John Henton FRCS(Plast), Consultant Plastic Surgeon
Published: 5 May 2026
Quick Summary: Lipoedema is a chronic disorder of abnormal fat deposition that is symmetrical, painful, and resistant to diet and exercise. Lymphoedema is a disorder of lymphatic drainage that causes fluid-based swelling, typically in one limb. They are distinct conditions with different causes, different clinical features, and different treatments — though they can and do overlap, a combination known as lipo-lymphoedema. Getting the diagnosis right before any treatment decision is not a formality; it changes everything about how a patient should be managed.
What is lipoedema?
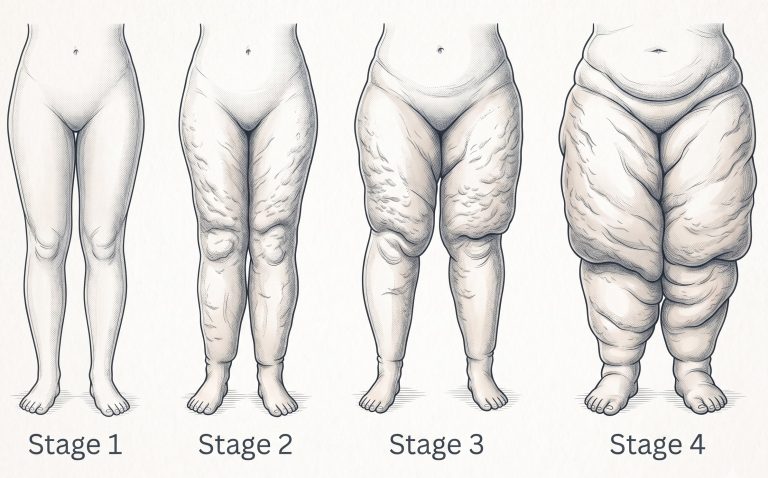
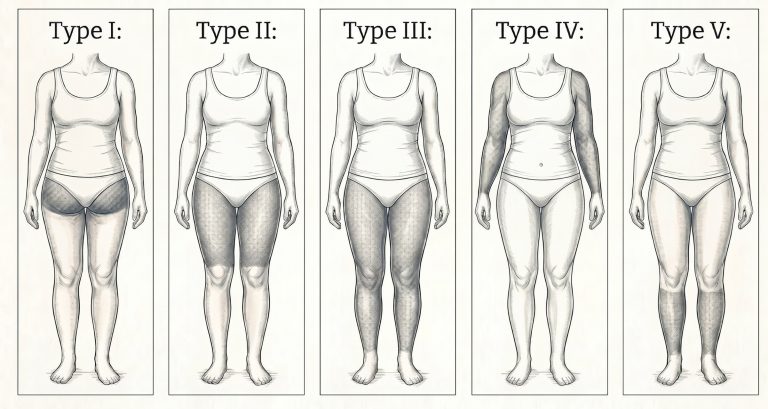
Lipoedema affects almost exclusively women and involves an abnormal, disproportionate accumulation of subcutaneous fat — most commonly in the legs, thighs, hips, and buttocks, and sometimes the arms. The fat is structurally different from ordinary adipose tissue: it is inflamed, hypersensitive, and poorly responsive to caloric restriction or physical activity.
Patients often describe a heavy, achy sensation, easy bruising, and pain to light touch or pressure. The feet and hands are characteristically spared, creating a distinct demarcation at the ankle or wrist. Many women with lipoedema have spent years being told they simply need to lose weight — which is both medically inaccurate and deeply unhelpful.
What is lymphoedema?
Lymphoedema results from failure or insufficiency of the lymphatic drainage system, causing protein-rich interstitial fluid to accumulate in the tissues. It is classified as primary (arising from a developmental abnormality of the lymphatic system) or secondary (arising from external damage — most commonly surgery, radiotherapy, infection, or trauma). It can affect any limb and, less commonly, the trunk, head, or genitalia. Unlike lipoedema, it often presents asymmetrically, and the swelling is fluid-based rather than fat-based. Without adequate treatment, chronic lymphoedema causes progressive fibrosis and increases the risk of recurrent cellulitis, which further damages the lymphatic system.
Comparison at a glance
| Feature | Lipoedema | Lymphoedema |
|---|---|---|
| Cause | Abnormal subcutaneous fat deposition; likely hormonal and genetic | Lymphatic insufficiency/obstruction: primary (developmental) or secondary (acquired) |
| Typical distribution | Legs, thighs, buttocks, and sometimes arms; feet and hands spared | One or more limbs; trunk; can affect hands and feet |
| Symmetry | Bilateral and symmetrical | Often unilateral or asymmetrical; bilateral possible |
| Pain | Common; disproportionate tenderness to palpation and easy bruising | Variable; heaviness and tightness more typical than tenderness |
| Pitting oedema | Absent in early stages; may develop if lymphoedema supervenes | Present, particularly in earlier or predominantly fluid-based stages |
| Stemmer’s sign | Negative (skin folds on toes and fingers can be lifted) | Positive (skin fold cannot be lifted — a reliable clinical marker) |
| Response to diet / exercise | Resistant; abnormal fat does not reduce with caloric deficit | Swelling reduces somewhat with elevation, compression, and MLD |
| Gender prevalence | Almost exclusively women | Affects men and women; secondary form follows the pattern of the causative event |
| Treatment approach | Conservative: compression, aquatic exercise. Surgical: tumescent liposuction | Conservative: MLD, compression. Surgical: LVA, VLNT, LYMPHA / ILR |

Lipo-lymphoedema: when the two conditions overlap
Lipoedema and lymphoedema are not mutually exclusive. In moderate to advanced lipoedema, the increased volume and structural disruption of affected tissue can impair local lymphatic drainage, giving rise to a combined condition: lipo-lymphoedema. This is not simply a coincidence of two separate diagnoses — the abnormal fat in lipoedema is thought to physically compress lymphatic channels and alter the microenvironment in ways that reduce lymphatic transport capacity.
Lipo-lymphoedema changes the treatment algorithm in meaningful ways. Surgical management of lipoedema by tumescent liposuction must be planned with awareness of the lymphatic component, as inadequate attention to lymphatic anatomy can worsen the lymphoedema. Conversely, a patient who appears to have straightforward lymphoedema may have an underlying lipoedema component that, if unaddressed, will limit the benefit of lymphatic reconstruction.
Accurate diagnosis before any surgical intervention is therefore not optional. Treating only the component that is most visible — rather than the one that is most important — risks incomplete outcomes and, in some cases, unnecessary harm. This is one reason why assessment at a specialist unit capable of evaluating both conditions simultaneously is of particular value.
The role of ICG lymphography
Indocyanine green (ICG) lymphography is a near-infrared imaging technique that maps superficial lymphatic flow in real time, following the intradermal injection of a small volume of ICG dye. It is safe, minimally invasive, and highly informative.
In cases where the clinical picture is unclear — for example, bilateral leg swelling with features of both lipoedema and lymphoedema — ICG lymphography can demonstrate whether lymphatic transport is impaired, and if so, to what degree and in which anatomical territories. It can distinguish linear (normal) from dermal backflow (abnormal) patterns, providing objective evidence of lymphatic dysfunction that clinical examination alone cannot reliably supply.
ICG lymphography is also used to map the anatomy ahead of lymphaticovenular anastomosis (LVA) surgery, identifying functional lymphatic vessels suitable for bypass. At the Great North Lymphatic Centre, ICG lymphography is central to the diagnostic and surgical planning pathway for both lymphoedema and suspected lipo-lymphoedema.
Frequently asked questions
Can lipoedema turn into lymphoedema?
Lipoedema does not transform into lymphoedema, but it can cause lymphoedema to develop over time. The accumulation of abnormal fat tissue can progressively impair local lymphatic drainage, eventually producing lipo-lymphoedema. This is one reason why earlier diagnosis and management of lipoedema is preferable — it may reduce the risk of a secondary lymphatic component developing.
Why was I told I just need to lose weight?
Lipoedema remains significantly underdiagnosed, and the presentation — disproportionate fat on the lower body — is frequently misattributed to obesity or poor lifestyle. The critical distinction is that lipoedema-related fat does not respond to caloric restriction or exercise, a defining clinical feature that separates it from ordinary adiposity. Many patients receive this advice repeatedly before being seen by a clinician with specific expertise in the condition.
How do I get a proper diagnosis?
Diagnosis begins with a structured clinical assessment by a clinician experienced in both conditions — ideally supported by objective imaging such as ICG lymphography where there is diagnostic uncertainty. If you are unsure whether you have lipoedema, lymphoedema, or a combination of both, the Great North Lymphatic Centre offers assessment specifically designed for patients in this position, without the need for a pre-existing diagnosis before referral.
About the Great North Lymphatic Centre
The Great North Lymphatic Centre is a specialist private practice based in Newcastle upon Tyne, led by Mr Chad Chang and Mr John Henton, both consultant surgeons with subspecialty expertise in lymphatic disease and reconstructive microsurgery.
The centre offers dedicated surgical pathways for lymphoedema (including LVA, vascularised lymph node transfer, and immediate lymphatic reconstruction) and for lipoedema, as well as a combined assessment pathway for patients with suspected lipo-lymphoedema or diagnostic uncertainty. ICG lymphography is available as part of the diagnostic workup. The aim is to give patients who have not found a definitive pathway through NHS services access to specialist assessment and, where appropriate, surgical treatment.
Your Next steps
If you are unsure whether you have lipoedema, lymphoedema, or a combination of both, the starting point is a specialist consultation.
If you would like to discuss your specific symptoms or arrange an assessment , please contact Great North Lymphatic Centre (GNLC), to schedule a consultation. You do not need to have a confirmed diagnosis before making contact.
Disclaimer: This content is for educational purposes only and does not constitute personal medical advice. Content written by Mr Chad Chang and peer-reviewed by Mr John Henton.