Blog

Author: Mr Chad Chang FRCS(Plast), Consultant Plastic Surgeon
Review Status: Peer-reviewed by Mr John Henton FRCS(Plast), Consultant Plastic Surgeon
Published: 20 March 2026
Quick Summary: Persistent swelling, a sensation of heaviness, or unexplained limb discomfort often indicates a failing lymphatic system. Understanding how this network works is the essential first step toward effective management. This guide examines how a healthy lymphatic system operates, what occurs in lymphoedema, and how the “gold standard” of lymphatic care helps you take control of your condition.
What is the function of the lymphatic drainage system?
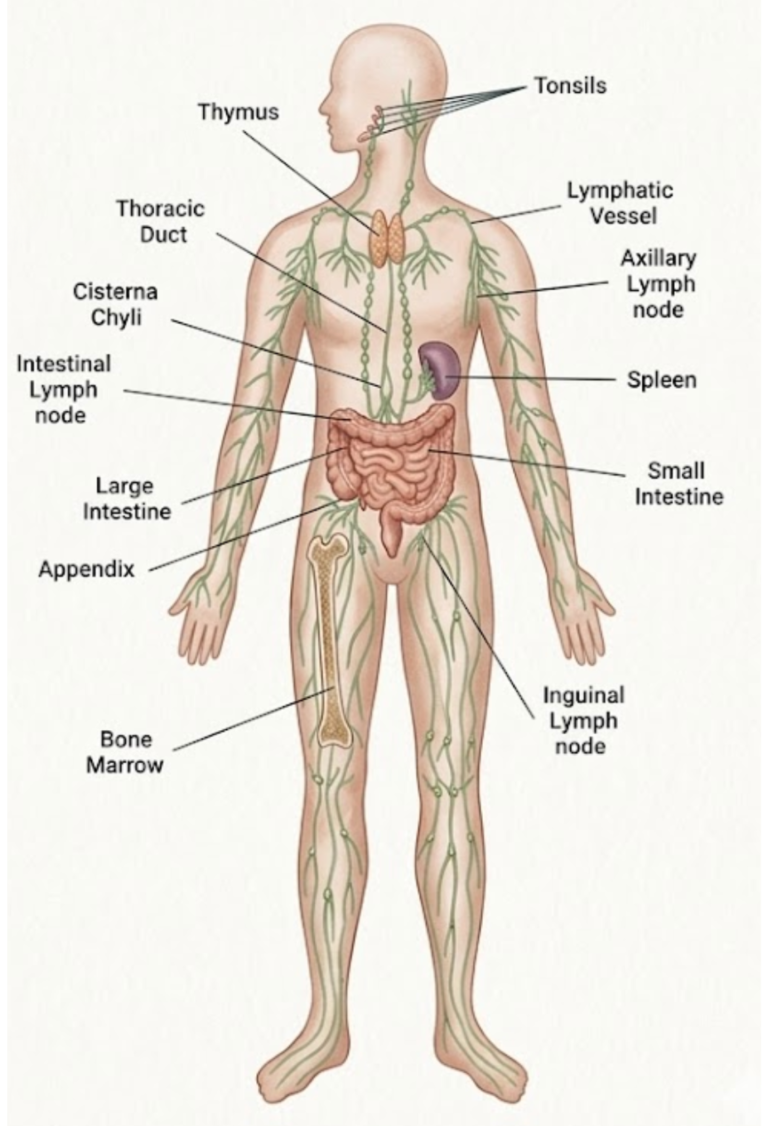
The lymphatic system acts as your body’s dedicated recycling and salvage network.
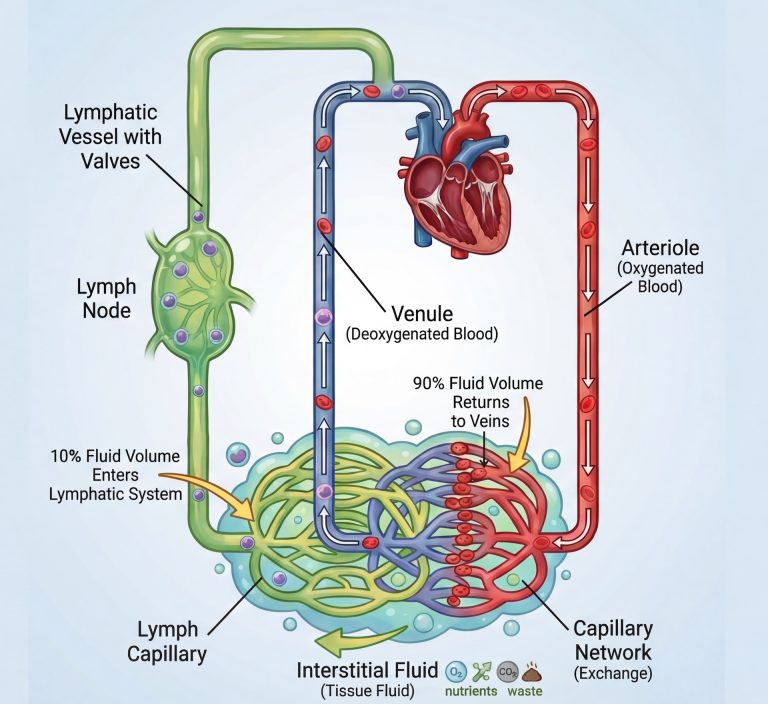
It works in constant partnership with the blood circulation rather than operating in isolation.
As blood pumps from the heart into the tissues, the veins are responsible for returning approximately 90% of that fluid. The remaining 10% is a protein-rich fluid left in the spaces between cells, known as the interstitium.
Because this fluid is “thick” with proteins and waste, it cannot fit back into the veins. The lymphatic system must step in to recycle this fluid and return it to your circulation:
- Collection: Tiny lymphatic vessels act like a sponge, soaking up this leftover fluid (now called lymph).
- Filtration: As the fluid travels, it passes through lymph nodes. These act as security checkpoints. Here, the immune system filters the lymph , identifying and neutralising threats like bacteria or viruses.
- The Return: Finally, the lymph fluid is emptied back into the large veins near the heart. This process is what prevents your tissues from swelling and keeps your immune system alerted to threats.
What exactly is lymphoedema?
Lymphoedema occurs when this lymphatic network fails. When the system cannot drain fluid adequately, it builds up in the tissues. This is not merely water; it is a protein-rich fluid that triggers chronic inflammation if it stays still for too long.
Over time, untreated lymphoedema results in:
- Persistent Swelling: This often begins in the hands or feet as the fluid “pools” at the furthest points of the limb.
- Infection Risk: Stagnant lymph is a perfect breeding ground for bacteria, leading to recurrent cellulitis (painful skin infections). These infections are particularly dangerous because they create a “vicious cycle”, where the infection causes more inflammation and further damages the remaining lymphatic vessels, making the swelling worse.
- Tissue Changes: Because lymph is rich in protein, your body identifies its presence in the tissues as a signal of injury. This triggers a state of chronic inflammation. In response, the body begins to lay down extra collagen (scar tissue) and store more fat in the affected area. This dual process of fibrosis (permanent hardening) and adipogenesis (fat growth) is why a limb that once felt “soft” and fluid-filled eventually becomes firm or “woody” to the touch.
- Skin Changes (Lymphorrhea): Ongoing chronic inflammation causes the skin to lose its natural health. It may become thick, leathery, or prone to leakage, known as lymphorrhea (fluid seeping directly through the skin).
How do I identify my stage of lymphoedema
Lymphoedema is a progressive condition. Identifying your stage early is the most important factor in successful treatment. Use the following guide to help identify your current symptoms and the corresponding “window of opportunity” for modern treatment.
| Stage | What You Feel & See | The Self-Check | The Surgical Window |
|---|---|---|---|
| Stage 0 (Sub-clinical) | The limb looks normal, but you feel “heaviness,” “tightness,” or aching at the end of the day. | No visible swelling, but jewellery or clothes feel tighter than usual. | Surgery is unlikely to be beneficial at this stage. Focus is on compression and MLD. Early ICG mapping can identify early drainage issues to guide therapy. |
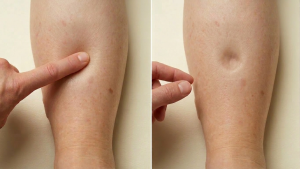
| Stage 1 (Reversible) | Visible swelling that improves or disappears after elevation or a night’s sleep. | The Pitting Test: Press your thumb in for 5s. It leaves a deep, clear “dent” or pit in the soft fluid. | This is the ideal time for physiological surgery (LVA), as the fluid is still “soft” and easy to bypass. |
| Stage 2 (Irreversible) | Swelling is constant and no longer improves with sleep. The limb starts to feel “woody” or firm. | Stemmer’s Sign: You can no longer pinch a fold of skin at the base of your toe or finger. Pitting becomes shallow or disappears. | Surgery is still highly effective but may require a combination of LVA, VLNT and liposuction to address co-existing fluid and solid tissue. |
| Stage 3 (Advanced) | Swelling significantly larger and heavy. Skin may become leathery, dark, or develop small growths. | Solid Tissue: The skin no longer “pits” due to fat and scar tissue. Fluid may leak from the skin (lymphorrhea). | The focus for surgery shifts to removing solid bulk through specialised liposuction or targeted debulking to restore comfort and mobility. |

The Importance of the "Pitting" Test
In the early stages, the swelling is mostly fluid. If you press your thumb firmly into the skin, it leaves a temporary dent. As the skin changes and fibrosis (hardening) sets in, the swelling becomes too firm to “pit.” This transition is a critical clinical sign that the condition is progressing from a fluid problem to a permanent tissue problem.
How do I perform the Stemmer’s Test?
The Stemmer’s test is a practical way to check for lymphoedema. While not a definitive medical diagnosis on its own, it helps providing some insights into your disease stage.
- Compare: Always compare your affected limb to your healthy side.
- Pinch: Attempt to pinch and lift a skin fold at the base of your second toe or middle finger.
- The Assessment:
- Negative (Normal): You can easily lift a thin fold of skin.
- Positive (Early disease): You may still be able to lift the skin, but it feels significantly thicker or stiffer compared to your healthy side.
- Positive (Stage 2+): The skin is too thick or “woody” to pinch at all. This suggest that your lymphoedema may be transitioning to a fibrosis dominant condition

What is the difference between primary and secondary lymphoedema?
Clinical management depends on whether the failure is from a developmental issue (how you were born) or acquired damage (external injury).
Secondary Lymphoedema (The Obstruction)
This is the most common form, typically caused by external injury to a structurally normal system. It occurs when a previously healthy network is damaged.
- Damage to the “Filters” (Lymph Nodes): This often occurs during cancer treatment, such as surgery to remove nodes or radiotherapy (radiation treatment). When a node is removed or scarred, the “cleansing” and “passage” of fluid stop at that point. Because the fluid has nowhere to go, it begins to build back up in the lymphatic vessel and leak back into the limb tissues.
- Damage to the “Pipes” (Lymphatic Vessels): This can be caused by major trauma, surgery, or severe infections. If a vessel is cut or scarred, the flow is blocked. Much like a blocked pipe in a house, the fluid behind the injury site has no choice but to leak into the surrounding tissues
Primary Lymphoedema (The Malformation)
In this form, the lymphatic system developed differently in the womb. The “plumbing” was never fully functional from the start. This typically involves vessels that are:
- Aplasia: Missing entirely.
- Hypoplasia: Underdeveloped or too narrow to handle the necessary fluid volume.
- Hyperplasia: Formed incorrectly—often too wide—which causes the internal valves to fail. This leads to reflux (fluid flowing backwards) instead of moving toward the heart.
Why this matters for your treatment
Because the underlying cause is different, the surgical strategy is different. For early secondary lymphoedema, we often can focus on “bypassing” a specific blockage (LVA) by connecting lymphatic vessels to nearby veins. For early primary cases, we may need to “replace” the non-functioning system by moving healthy lymph nodes from another part of the body (VLNT). However, if fibrosis has set in and your lymphoedema is predominantly solid tissue, neither option is suitable, and we must physically remove the fibrosis using specialised liposuction.
How is lymphoedema managed without surgery?
The gold standard for non-surgical management is Complete Decongestive Therapy (CDT). This multi-modal approach focuses on manually assisting the compromised system to move fluid and prevent tissue damage.
The Four Pillars of Decongestive Therapy
- Manual Lymphatic Drainage (MLD) A specialised, gentle massage using specific rhythmic movements to stimulate lymphatic collectors. It aims to guide fluid away from congested areas by directing lymph toward working drainage routes and nodes.
- Exercise and the ‘Muscle Pump’ Unlike blood, lymph has no central heart to pump it; it relies on the contraction of surrounding muscles. Movement acts as a natural pump to propel fluid out of the limb. Resistance training and swimming are highly beneficial when combined with compression.
- Compression Therapy The use of medical-grade garments (sleeves, stockings) or multi-layer bandages to apply external pressure. Compression works in two ways: (1) it provides a firm wall for muscles to push against, sandwiching the lymphatic vessels and making the muscle pump work more efficiently; (2) the increased pressure outside the vessels makes it physically harder for lymph to leak out into your tissues.
- Intensive Skincare Lymphoedematous skin is often fragile and stretched, making it prone to microscopic cracks. Daily hydration seals the skin barrier, serving as a primary defence against bacteria entering the tissue and triggering cellulitis.
When is conservative management not enough?
Complete Decongestive Therapy (CDT) is the essential foundation of care, but it is a maintenance strategy designed to manage symptoms rather than a structural repair of the lymphatic system. For many, the daily requirement for high-grade compression and the persistent threat of infection remain significant challenges that CDT alone cannot resolve.
In specialist practice, we identify “windows of opportunity” where surgical intervention can modify the course of your lymphoedema. You may wish to consider a surgical assessment if you experience:
- Recurrent Cellulitis: Even a single infection can trigger further inflammatory damage to the remaining lymphatic vessels, worsening the underlying failure.
- Static or Increasing Volume: When limb swelling fails to improve or continues to progress despite a consistent, high-grade compression regime.
- Significant Lifestyle Impact: When the physical and mental effort required for lifelong conservative care becomes difficult to sustain.
The Role of Modern Imaging
To move from general management to a precision-planned surgical approach, we utilise ICG Lymphography. By injecting a near-infrared fluorescent dye, we can map your lymphatic network in real-time. This technology allows us to see exactly which vessels are actively pumping and where drainage is obstructed.
This visual information is essential for identifying the most effective surgical path, whether that involves creating a physiological bypass (LVA), transferring new nodes (VLNT), or physically removing solid tissue through specialised liposuction.
If you would like to discuss your specific symptoms or arrange an ICG Lymphography assessment to map your drainage, please contact Great North Lymphatic Centre (GNLC), to schedule a consultation.
Disclaimer: This content is for educational purposes only and does not constitute personal medical advice. Content written by Mr Chad Chang and peer-reviewed by Mr John Henton.